Why Sepsis Matters
Sepsis is the third leading cause of death in U.S. hospitals, contributing to at least 350,000 deaths annually. Globally, sepsis accounts for nearly 1 in 5 deaths. One in three patients who die in a hospital had sepsis during their stay.
Early detection saves lives, but existing tools fail to give clinicians the confidence they need to act on alerts.
Sources: WHO, AAMC
The Problem with Current Tools
Trust. Clinicians can't see the underlying data that the model uses to make predictions.
Since they are unable to see the full picture, they do not have full confidence in the alerts.
False negatives vs. false positives. Sepsis prediction models are excessively tuned to
reduce false negatives as missing a patient with sepsis has much more severe consequences. However, ignoring
false positives causes an increased number of alerts and, subsequently, clinicians are overwhelmed
leading to less trust in the alerts.
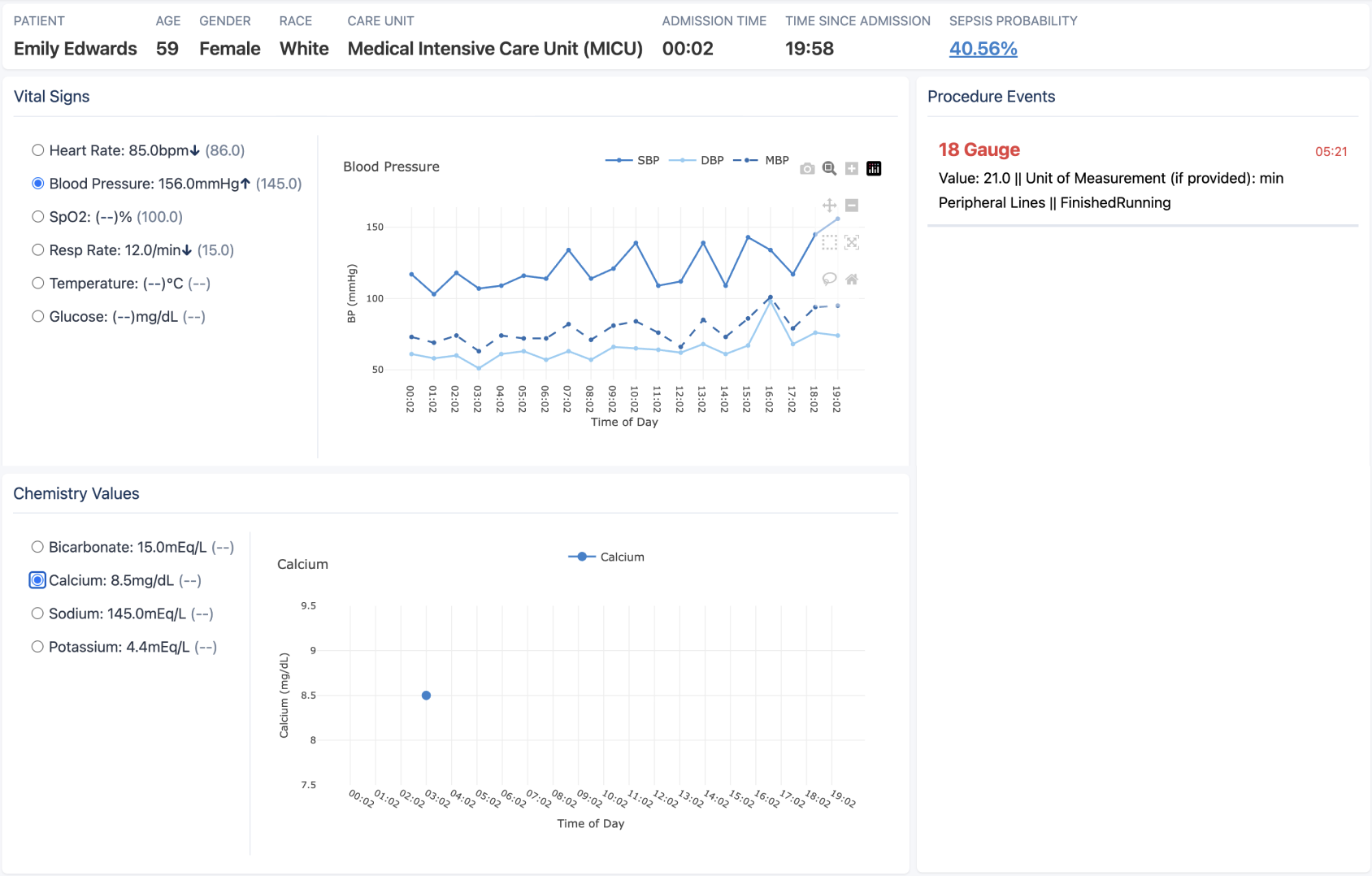
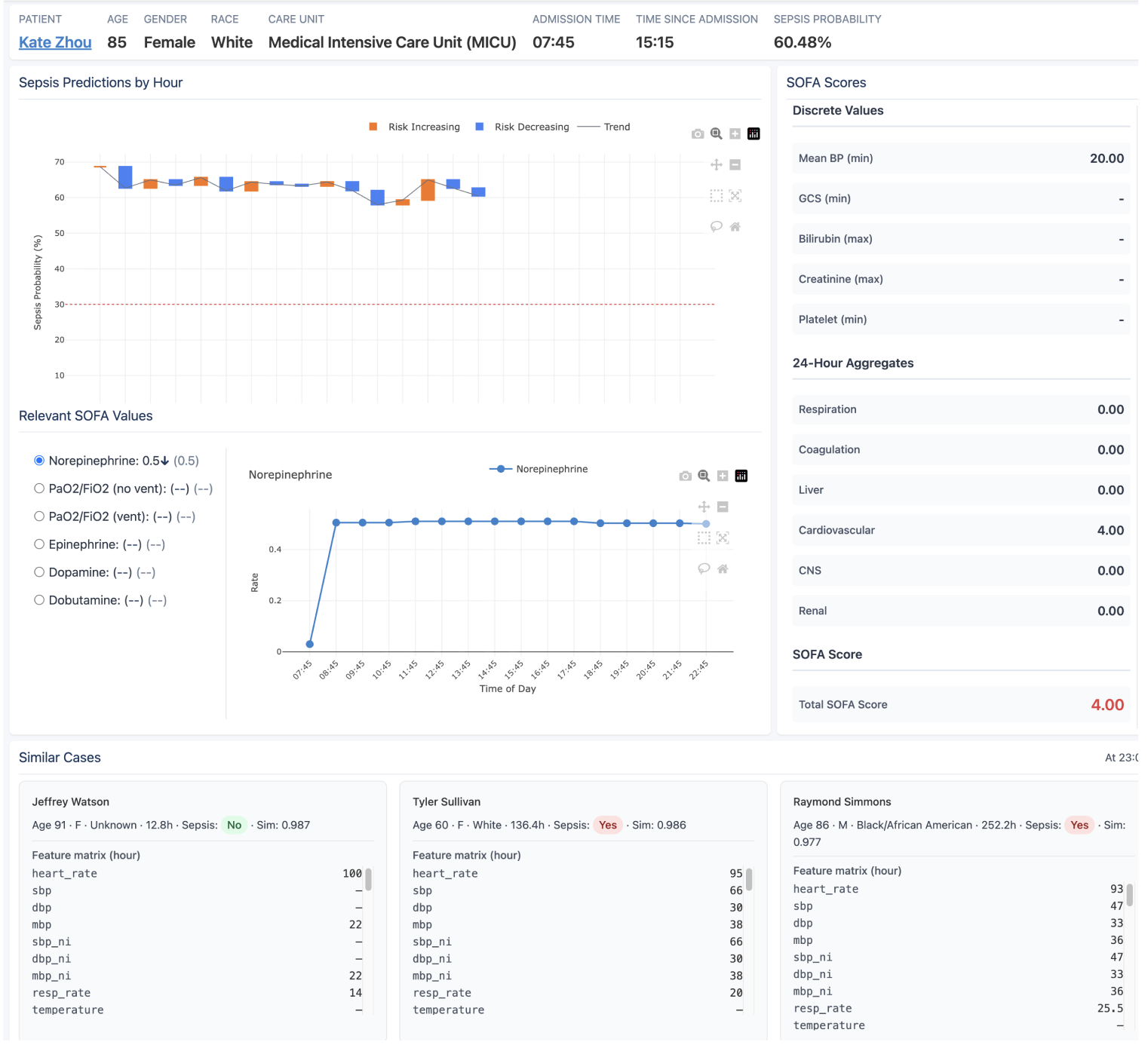
What We Built
A clinician-facing sepsis prediction and decision support system. It shows the data behind every alert—vitals, procedures, and risk trends—so clinicians can see exactly what the model sees and decide whether to act.